
PROTEUS trial
A trial that raises more questions than it answers.

The PROTEUS trial reports that the addition of apalutamide to perioperative androgen-deprivation therapy (ADT) improves both co-primary endpoints in men with high-risk localized or locally advanced prostate cancer undergoing radical prostatectomy. The study is large, double-blind, and well conducted, and it establishes that androgen-receptor pathway inhibition is biologically active in this setting. Whether it should change practice is a separate question, and the answer is less settled than the trial’s positive headline suggests. Two design choices—the comparator and the endpoints on which the result principally rests—operate in the same direction, and their combined effect is to make a genuine but modest signal appear more robust, and more clinically established.
The comparator does not correspond to the clinical decision.
All patients in PROTEUS received perioperative ADT; the trial evaluated only the incremental contribution of apalutamide to that backbone. As the investigators acknowledge, perioperative ADT itself represents an intensification beyond current guideline recommendations, under which most of these men would undergo prostatectomy alone, with adjuvant or salvage therapy reserved for relapse. The trial, therefore, addresses whether apalutamide adds to ADT, not whether the combined strategy is superior to standard care. The comparison against surgery alone is being conducted separately and is not part of the present registrational result. This is a defensible design—a pathological endpoint is uninterpretable without systemic therapy in both arms, and an active control preserves blinding—but it has consequences that shift outcomes in a more favorable direction. Because both arms are castrated, the toxicities of ADT are common to both, thus narrowing the difference between the two groups, misleading the reader to think there is no added toxicity to their “standard-of-care”. Meanwhile, in reality, surgery alone can already have a great negative impact on quality of life, let alone adding the toxicity of ADT and apalutamide to this.
The pathological co-primary endpoint: prognostic, but not a basis for treatment decisions
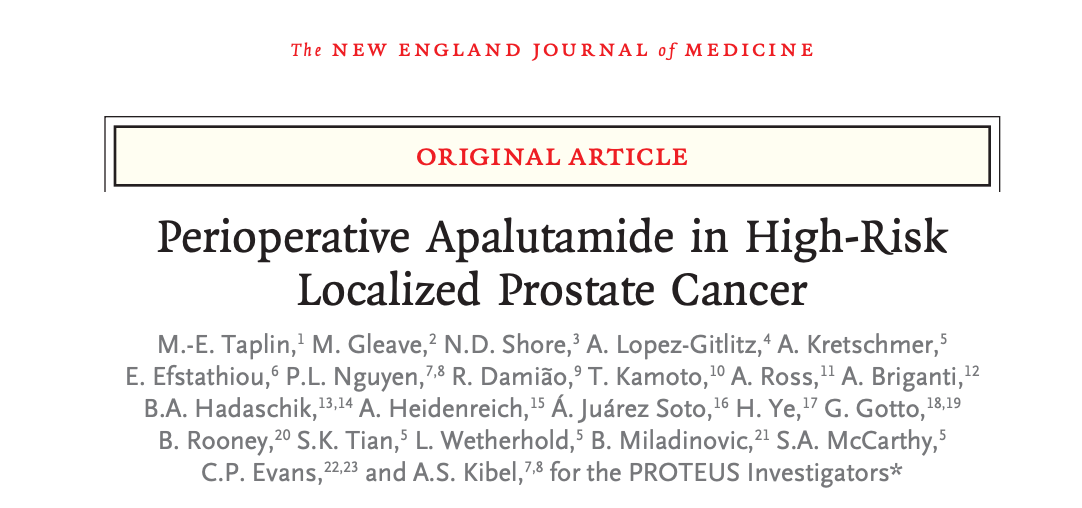
This is the crux of the trial’s interpretation. The composite of pathological complete response or minimal residual disease (pCR/MRD) was markedly more frequent with apalutamide—roughly nine times as frequent—and within PROTEUS the presence of minimal residual disease was strongly associated with subsequent metastasis-free survival. This establishes the endpoint as prognostic. It does not establish it as a basis for clinical decision-making, and the two are not the same.
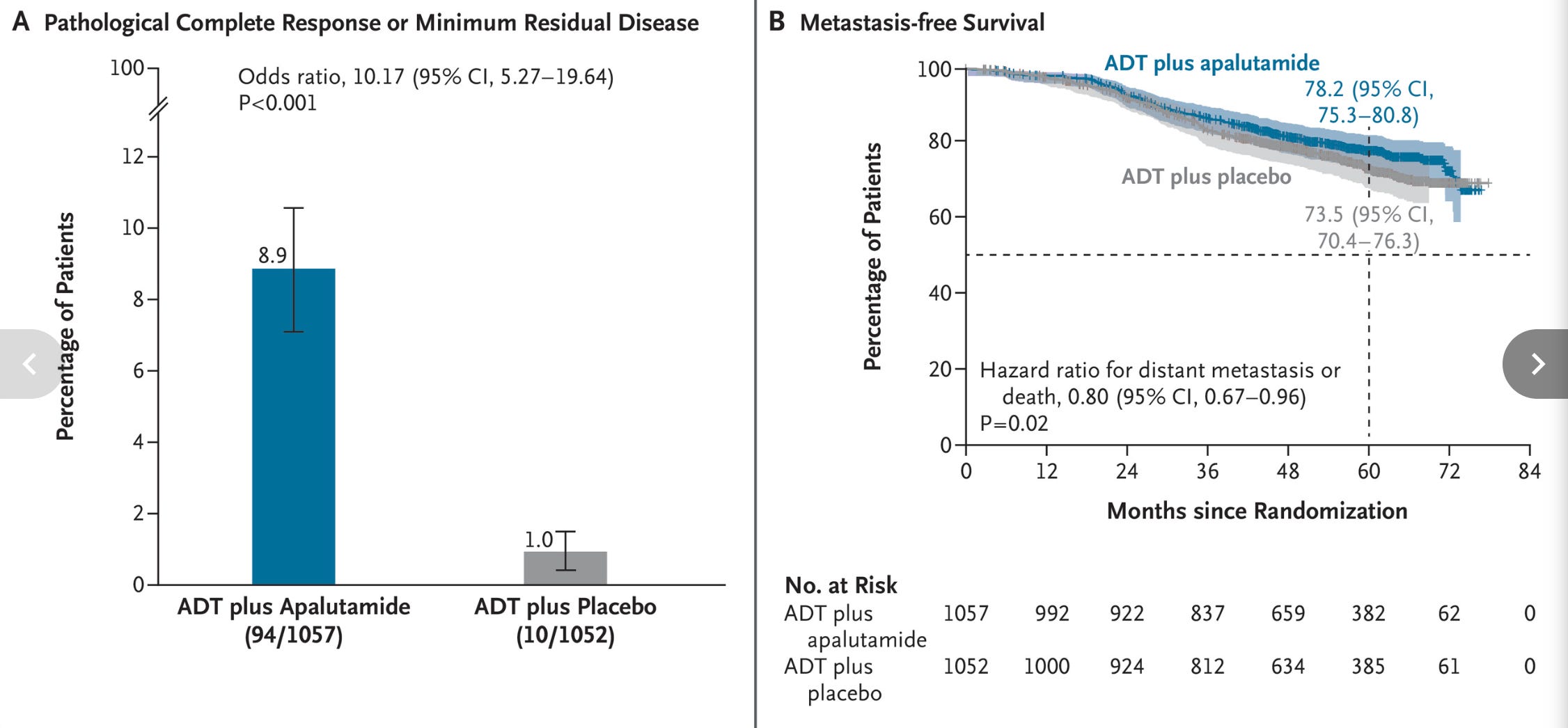
A prognostic marker stratifies patients by risk; a surrogate endpoint makes the stronger claim that a treatment effect measured on the marker reliably predicts a treatment effect on the clinical outcome. The inference required to justify pCR/MRD as a co-primary efficacy endpoint is the latter, and it has not been demonstrated. But there is a more immediate, and arguably more important, limitation. Pathological response is observable only after treatment, in the prostatectomy specimen; it cannot exist in a patient who has not received neoadjuvant systemic therapy, and it cannot be predicted before treatment is given. The trial offers no way to identify, in advance, the minority of men—fewer than one in ten—who will achieve minimal residual disease. The favorable outcomes of that subgroup are therefore recognized only in retrospect, once the treatment decision has been made and its toxicity incurred. The whole cohort is committed to a year of ADT plus apalutamide so that a small, post-hoc-identifiable fraction may benefit. That the achievement of minimal residual disease is associated with better metastasis-free survival is genuinely encouraging for those patients; it does not inform the patient or the clinician whether this is the optimal treatment for any specific individual.
The consequence is that the endpoint that produced the trial’s most striking numerical result is also the endpoint least able to direct care in real-life setting. It does however teach us post-hoc that reaching pCR and/or MRD has a beneficial impact on MFS, but there is no way to know who will reach pCR/MRD and who will not BEFORE surgery.
The validated endpoint was not met on the basis on which it was validated
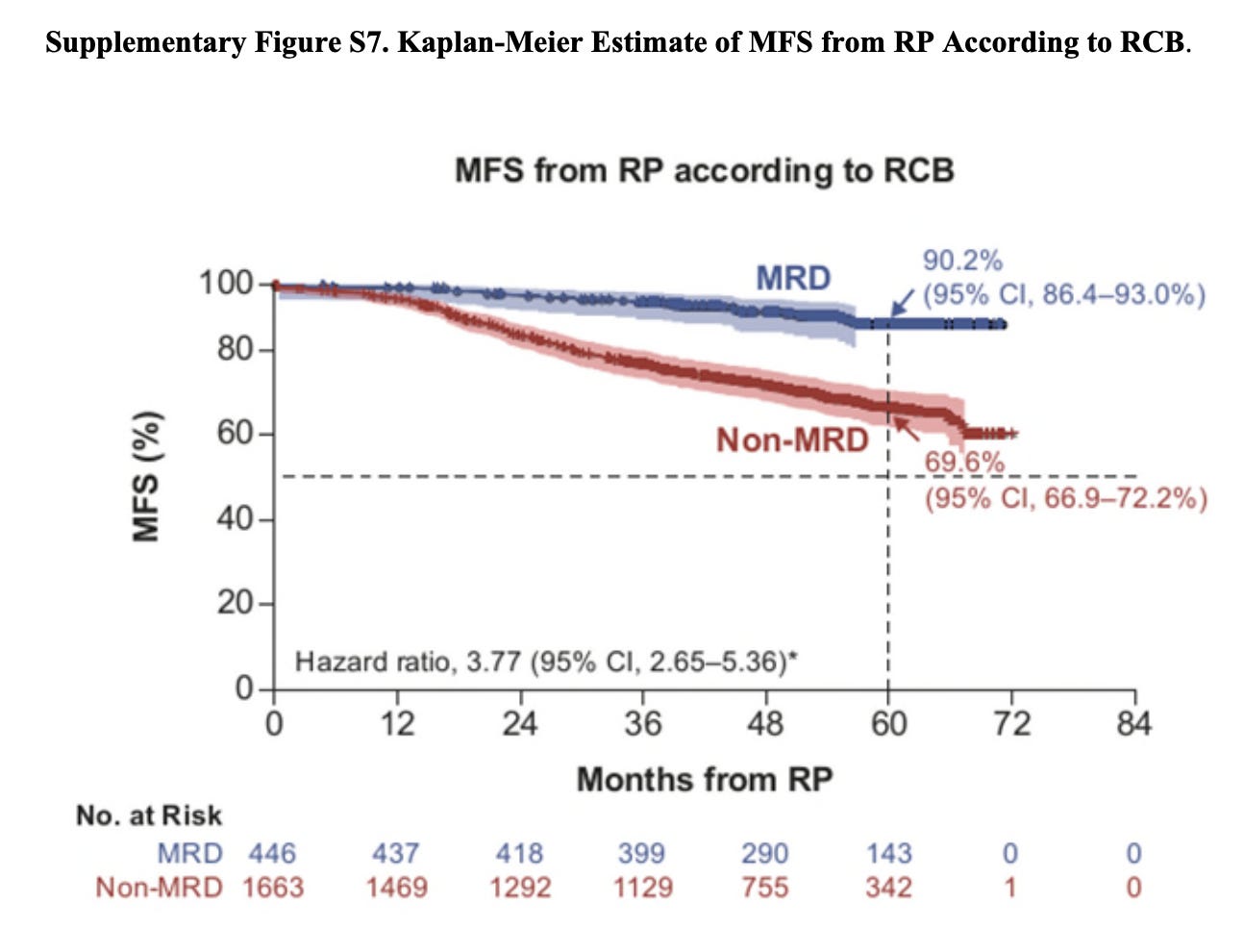
Of the two co-primary endpoints, only metastasis-free survival has an established surrogate relationship to overall survival in localized prostate cancer, and that relationship was demonstrated using conventional imaging. In PROTEUS, metastasis-free survival assessed by conventional imaging alone did not reach statistical significance. Significance was achieved only when lesions detected by prostate-specific membrane antigen positron-emission tomography (PSMA-PET) were incorporated—a modality of greater sensitivity that detects metastatic disease earlier and at lower burden than the imaging on which the surrogacy of metastasis-free survival was established, and one introduced into the trial after its inception. The positive primary result therefore rests on a definition of the endpoint whose relationship to survival has not been validated, while the validated definition (metastasis-free survival assessed by conventional imaging, the basis on which ICECaP established its surrogacy for overall survival) yielded a result that did not cross the conventional threshold for significance.
The most patient-relevant benefit
The most clinically meaningful signal in PROTEUS may be the delay in time to subsequent therapy: a median of 33 months, achieved with one year of added treatment and, on current and still immature data, no accompanying difference in overall survival.
Interpreting this benefit requires understanding what therapy-free time means in this disease. High-risk prostate cancer that recurs after prostatectomy is, for most men, managed rather than cured. Once intensified systemic therapy is begun, it is rarely stopped: a patient who responds and then progresses moves through successive lines of treatment, and short of electing best supportive care, he remains on systemic therapy of one form or another for the rest of his life. Each of these treatments carries its own burden. The clinically relevant currency in this setting is therefore not only how long a man lives, but how much of that life precedes the point at which uninterrupted systemic therapy begins. A delay in starting that therapy is a delay in the onset of that burden.
Read this way, the trial’s findings cohere. If overall survival is unchanged but the time to subsequent therapy is extended by years, the principal effect of moving intensification to the front is to redistribute when a man spends his treatment time, not to extend his life. He receives a defined course of therapy early, then enjoys a longer interval free of it, rather than beginning open-ended therapy sooner and remaining on it. For many patients, this is a real and desirable trade, and it may be the most patient-relevant outcome the trial produced.
Conclusion
PROTEUS demonstrates convincingly that apalutamide is active when added to perioperative ADT. Its most tangible benefit may be a substantial delay in the need for subsequent therapy—on current data, time away from treatment rather than additional time alive—which, for many patients, is a meaningful gain in its own right. But the trial’s claims are narrower than its positive framing conveys. The benefit is measured against a comparator that does not represent standard care; it is anchored to a pathological endpoint that is prognostic but cannot guide treatment selection, since it is identifiable only after the fact; and its one survival-linked endpoint, metastasis-free survival, reached significance only when assessed by PSMA-PET—not by the conventional imaging on which its surrogacy for overall survival was actually established. The comparator and the endpoints do not fail independently so much as they reinforce one another, lending an impression of established benefit to findings that, on present evidence, demonstrate biological activity but not yet clinical benefit. Before perioperative androgen-receptor inhibition is adopted into routine practice, it should be shown to improve outcomes that are known to matter, measured against the treatment that patients actually receive. PROTEUS was not designed to provide that demonstration, and its positive result should be read with that limitation firmly in view.